Discussion: Details on CVD Biomarker Laboratory Assessment and treatment using pharmaceutical drugs
Okay, I am a back to round up this topic by exposing you to some salient things about the biomarkers and how we measure them in the medical laboratory and as well, give you some heads up on how to easily identify drugs used for treatment and management of cardiovascular diseases (CVD). This is however for learning purpose and does not encourage you prescribing them to suspected people with any form of CVD. The consequences can be sure fatal!
In the last post, in general, we were able to understand that, the risk factors and causes of cardiovascular diseases included genetics (family based), age (mostly associated with old age), sex (susceptibility is higher in men are than women), cigarette smoking, physical inactivity, diet (high intake of saturated fats, and salt), chronic alcoholism, an existing cardiovascular event like heart attack, stress, radiation therapy, hypertension, diabetes and hypercholesterolemia.
I want to as this point add that, some serum markers like the production of homocysteine ( an amino acid) in the body can also contribute to CVD. This particular amino acid has been implicated in damaging blood vessels, increasing oxidative stress thereby leading to the development of high blood pressure. This however is not a traditional risk factor for CVD but it happens. This of course happens when the level of this amino acid is on the high side. Best way to knock its level down is by simply taking food that is rich in vitamin B (folic acid, B12, and B6) will go along way. In fact, balance diet is enough to avert this.
Let's briefly talk about how we actually diagnose
This area is of course my specialty. Correct diagnosis remains the bed rock for accurate treatment and management of any CVD. In the medical laboratory, what we look out for are those biomarkers associated with the condition, and are known to be either elevated or decreased. For example, anything that will make the enzyme Alanine transaminase, ALT aka Alanine aminotransferase to be increased in the body, definitely it points to one organ, the Liver! If then the enzyme Aspartate transaminase, AST is increased as well, then we can say that the problem is stemming from the mitochondrial of the liver.
This is just a simple way, biomarkers help us pin down a particular disease condition. Every biomarker always have their root, hence, a mastery of these biomarkers and their role in the body and their location makes it much easier to diagnose any disease condition. However, not all biomarkers are specific for a particular disease. Some biomarkers will only give a head-start and then you can now go further to do more test to actually know the root problem. So, when you receive a medical laboratory test request form containing a number of test to be conducted, is definitely for a reason - to rule out doubts.
Laboratory Diagnosis of Cardiovascular Diseases
The two major ways to diagnose CVD are through Laboratory testing (blood test) and Radiographical analysis in addition to Electrocardiogram, ECG. These are the main diagnostic procedures carried out for the detection of heart disease risks. Lipid panel (used to determine the level of fats in the individual) and blood sugar estimation are highly indispensable in the diagnosis of cardiovascular disease.

Blood sample of a patient with severe genetic hyperlipidaemia (excessive elevation in lipid/fats)
{kind=link}
In lipid profile/panel which is usually the first point of call to assess the risk, fats, cholesterol, LDL, HDL, VLDL, and triglycerides are tested while fasting. You can read more about these parameters in my previous post, the link to read about them are embedded there. Mere looking at the sample above, the upper part of the sample above the red coloured blood are fats. I need no prophet to tell me that this patient is sure suffering from hyperlipidemia. Running the lipid panel test, will further reveal which particular lipid is excessively elevated so that appropriate treatment pattern can quickly be designed.
You might want ask why do sugar test for someone at risk of CVD. High sugar (glucose) level in the blood tend to damage the blood vessels and nerves that mainly control heart functions. Remember, the heart is in contact with blood all the time. Once they continue to damage the blood vessels, this ultimately leads to increase in blood pressure beyond normal (hypertension). The constellation effects of all this ultimately results to CVD.
Usually, fasting blood sugar, Oral glucose tolerance test (OGTT), post prandial test are done to ascertain blood sugar status of the individual. While OGTT measures the patient's body response to glucose after the patient is given about 75-100 grams of glucose in a sweet drink. This test is usually performed in the morning after an overnight fast. Similarly with fasting blood sugar test. If all things being equal and the pancreas producing insulin is functional, it is expected that in in OGTT, the glucose level in the patient rises and then returns back to the physiologic level within 60 minutes (2Hours).
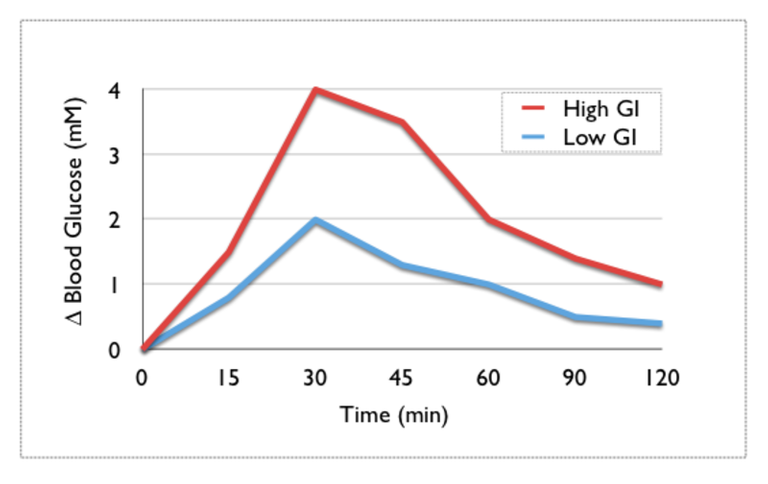
Illustration of the changes in blood glucose over time following a high and low GI carbohydrate
{kind=link}
If the concentration of glucose rises and then falls, it means that the excess glucose which is not needed by the body has been mopped up by insulin and converted to glycogen for storage. As can be observed in the graph above. In a situation where the concentration of glucose does not fall but continue to rise, it simply means that the patient is likely prediabetic or diabetic.
This test is not only important for assessment of CVD risk factor, but also in the assessment of prediabetes and diabetes in pregnant women. Pregnancy can induce a type of diabetes known as Gestational diabetes, so it is very important to go for this test as an expectant mother to avoid putting your child at risk of being obsessed, which of course can make delivery extremely difficult.
Finally on diabetes, besides the test above, Glycosylated haemoglobin concentration is also measured. This test mainly measures the amount of haemoglobin that have been bound by sugar molecules in the body over a period of about 3 months. The rationale behind this test is the fact that sugar molecules like glucose, fructose etc. spontaneously bind to the haemoglobin once they are present in the blood.
In essence, the higher their concentration, the higher the bind to the haemoglobin. Measuring the concentration of the of those bound to the haemoglobin and comparing their concentration with the reference value (normal value) will help determine if the patient is prediabetic or diabetic.

Looped MRI video of a healthy 13 year old female's heart beating
{kind=link}
Now on the aspect of radiological analysis and ECG. These procedures give a real time update on the state of the heart muscle. While radiological analysis focuses and relies on the principle of visual display inspection through production of live images. This images are then used to detect and identify any findings.
Ability to differentiate between a normal heart and abnormal one makes radiological procedures easier. The common examples are X-rays (shows shapes and sizes of heart, lungs and major blood vessels), Computed Tomography (CT or CAT scan that detects calcium deposits in the arteries), Magnetic Resonance Imaging (MRI, creates pictures of the heart), Ultrasound (US), Fluoroscopy and more.
ECG on the other hand is a test that measures the electrical activity of the heart. It records the heart's rhythm and activity on a moving strip of paper or a line on a screen. With ECG, you as well detect various heart conditions such as heart attacks, arrhythmias, and damage to the heart muscle.
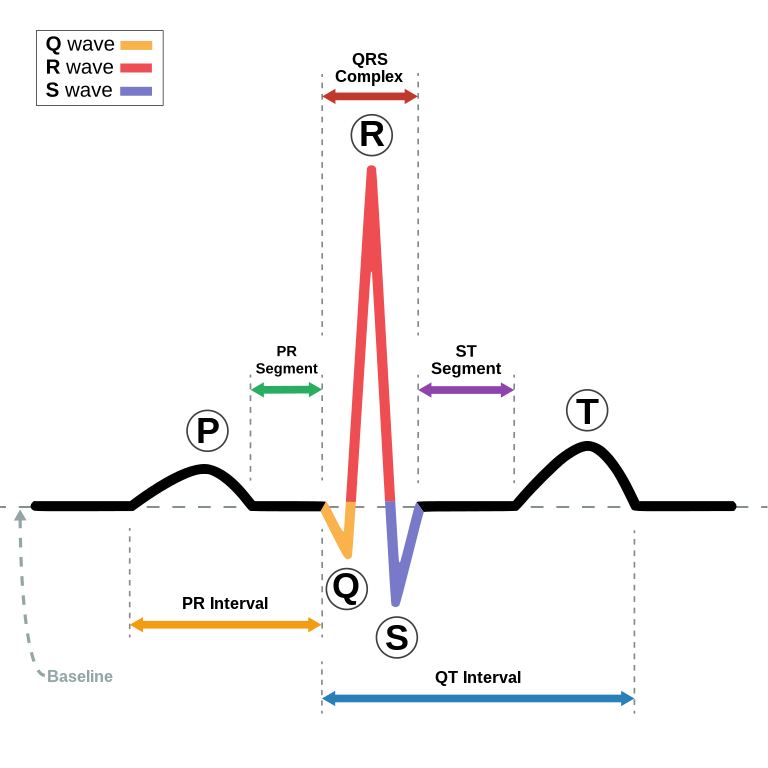
Schematic diagram of normal sinus rhythm for a human heart as seen on ECG
{kind=link}
The wave pattern on the paper or on the screen and it's interpretation simply dictates the state of the individual. There is another type called Echocardiography (this particularly creates a moving picture of the heart, so that it can be studied for any abnormality).
The Major specific Biomarkers associated with the heart and looked out for in CVD cases
When the heart muscle cells die or is injured severely during certain heart diseases, it is always accompanied by the release of proteins and molecules into the blood stream. These proteins such as the Cardiac Troponin, C-reactive protein, CRP (an acute phase protein that marks inflammation), apolipoproteinA1 etc. are mostly seen but CRP and cardiac troponin are most common.
C-reactive protein (CRP) are called acute phase protein mainly because their levels are remarkable raised during most inflammatory reactions in our body. Once they are seen elevated, it means that there is an inflammatory reaction going on. It is always an early sign of inflammation, hence, a major diagnostic factor. Atherosclerosis which have explain in the previous article as the an inflammatory disease that occurs due to damage to the endothelium of the blood vessels. This is no different in the heart and when it occurs, what is always observed is an elevation of CRP level.
It is important to know that, it is not the heart itself that produces this protein, rather, it is as a result of the released pro-inflammatory cytokines at the early stage of the disease which trigger the liver cells' hepatocytes to produce the CRP. In essence, CRP is produced in the liver and not in the heart. Once CRP is released, it can further stimulate macrophages to take up Low density Cholesterol (bad Cholesterol in the body) and their accumulation and plague formation.
How do we analyse these proteins in the laboratory?
Generally, most analyzers used for measuring biomarker levels are based on the principle of antigen / antibody interaction. Usually, one of them are known, and then you use the known to find the unknown. For example, the reaction well could be impregnated with the antigen of the solute we want to identify in a test sample. Since Antigens bind to antibodies, if the sample contains the antibody of interest to us, it will bind and form a complex and vice versa.
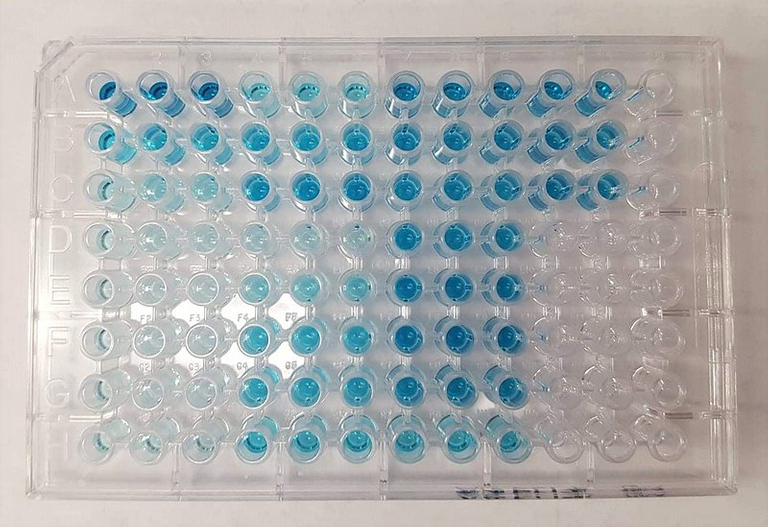
An ELISA (enzyme-linked immunosorbent assay) on a half-volume 96-well plate developed with a horseradish peroxidase secondary antibody and the colorimetric substrate TMB (3, 3', 5, 5'-tetramethylbenzidine) which reacts with the HRP to turn blue
{kind=link}
The complex is then identified through various means, say using a conjugate antibody to which an enzyme has been attached to. Enzymes will always react to the right substrate to produce a product. This product can be in the form of a colour change. The colour produced is them detected and measured.
The higher the intensity, the greater the amount of solute in the test sample and vice versa. This type is called the Enzyme linked Immunosorbent assay, ELISA. This can be used for the detection of many antigens or antibodies and not just restricted to CRP.
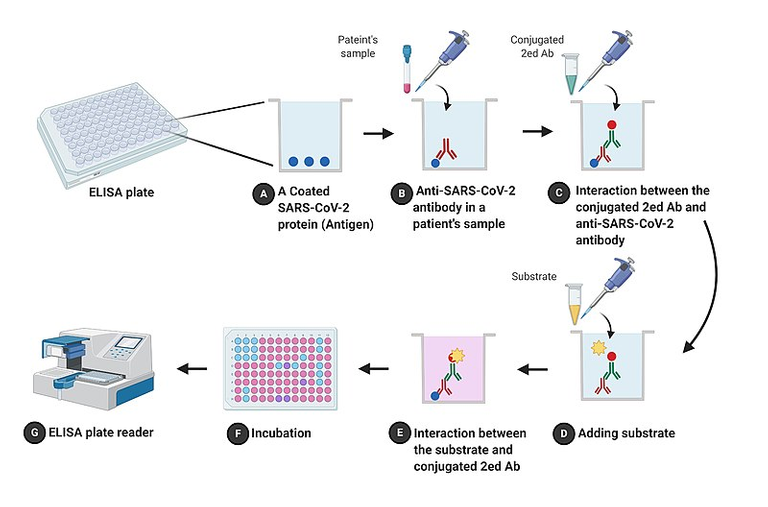
Schematic flowchart: ELISA and COVID-19 detection
{kind=link}
Likewise, some antibodies are also bound to fluorescent compounds (they can produce fluorescence light that can be detected and measured, this is called fluorescence immunoassay. Others also involve chemiluminescence reaction that give off characteristic colours when two reactant react. Lastly you could also have the radioimmunoassay, here radioactively labelled antibodies are used to detect an analyte in the sample. In this case, the analyte is CRP.
In he case of Cardiac Troponin I, the risk factor detected is that which is associated with myocardial infarction and cardiac muscle damage and injury. This protein is highly specific for the cardiac muscle and that's it is a dependable biomarker for CVD diagnosis. It's detection is similar with that of CRP I explained above.
Pharmaceutical drugs used for CVD treatment
The sole aim here is to help you understand the simple terminologies and how to identify drugs used for CVD management and treatment. The names of these drugs like we explained previously in the last article most is associated with the organ or they effect their action. For these drugs to target any organ, it means, that organ plays a role in causing the CVD or it's simply implicated.
For hypertension, they are called antihypertensive and they aim to lower the blood pressure and their a lot of them depending on where they exert their actions. For hypertension treatment, know this; Angiotensin converting enzyme inhibitors (ACEI) are always the first line treatment before any other drug is used, mainly in primary hypertenion (occurs when you have abnormally high blood pressure that's not the result of a medical condition but due to unhealthy life style). Knowledge of drugs and their mechanism of action during my pharmacology class back in those days of clinical classes have not failed me.

Pharmacological drugs
.jpg){kind=link}
I wouldn't want to go into the intricacies of these drugs but know this also; when you see any drug brand that has these names ramipril, quinapril, benzazepril, imidapril, they are all ACEI drugs. They mostly have the suffix -pril ending them. You also have the diuretics (thiazide and loop diuretics) such as spironolactone, metolazone bumetanide, torsemide, furosemide etc. They usually have the -ide and -one attached to their name.
Adrenoceptor antagonists: They are the Beta-blockers and alpha blockers. These drugs dramatically decrease heart rate and its contractility. They are better used when the patient is not responding to other antihypertensive drugs. You have metoprolol, esmolol and atenolol, labetalol. You also observe something common with them, the suffice -olol.
Next commonly used are the Angiotensin II receptor blockers. They more preferred to ACEI. You would also see most of them bear the name losartan, candesartan, eprosartan. Hope you also observed the suffix -sartan. Next is also the Calcium blockers. Calcium is needed for muscle contraction, so inhibition of calcium into the sarcoplasmic reticulum of the heart muscles will prevent contraction.
They are used in therapy for tachyarrhythmias and angina. You have amlodipine, barnidipine, cilnidipine, clevidipine, felodipine, isradipine. Hope you again observed the suffix -dipine.
Now the part that can be confusing is the Vasodilators, they relax the vascular smooth muscles in resistant blood vessels. You have the hydralazine and minoxidil. They seem to be the odds out. I could remember calling them the black sheep then. That way, I was able to remember them easily.
There are many more, of which if we decide to go into, this blog post will probably be too lengthy and maybe boring for non science enthusiast. So at this point, let's call it a day on everything that has to do with CVD diagnosis, laboratory assessment, and treatment using pharmaceutical drugs. I believe you should able to at least identify some of these drugs when next you see them.
Remember, constant exercise and the elimination of a sedentary life style are highly recommended for the maintenance of a healthy body mass index (BMI). cardiovascular disease when properly treated may not be life threatening and can be prevented in most cases with proper and healthy preventive measures.
I greet you pharmaceutically!
References
•Frequency of laboratory testing and associated abnormalities in patients with hypertension
•Assessing Screening Guidelines for Cardiovascular Disease Risk Factors using Routinely Collected Data
•Troponin and C-reactive protein have different relations to subsequent mortality and myocardial infarction after acute coronary syndrome: A GUSTO-IV substudy
•Hypertension
•Prediction for cardiovascular diseases based on laboratory data: An analysis of random forest model
•Essential Hypertension
•Antihypertensive Medications
•First‐line drugs for hypertension
Original version of this research work can be accessed here
I have missed reading your post.
Always so educating, lengthy but very educating.
I love the simplicity. 👌👍
HI @beulah4real, been busy with real life engagements. Decided to maximize this little break. Been a while you also.
You haven't been writing, you need inspirations to kick off?😉
I absolutely do. I'm sure il get it soon.
Alright great!
All the best and good luck.
Congratulations!
✅ Good job. Your post has been appreciated and has received support from CHESS BROTHERS ♔ 💪
♟ We invite you to use our hashtag #chessbrothers and learn more about us.
♟♟ You can also reach us on our Discord server and promote your posts there.
♟♟♟ Consider joining our curation trail so we work as a team and you get rewards automatically.
♞♟ Check out our @chessbrotherspro account to learn about the curation process carried out daily by our team.
🥇 If you want to earn profits with your HP delegation and support our project, we invite you to join the Master Investor plan. Here you can learn how to do it.
Kindly
The CHESS BROTHERS team
💕
Thanks for your contribution to the STEMsocial community. Feel free to join us on discord to get to know the rest of us!
Please consider delegating to the @stemsocial account (85% of the curation rewards are returned).
Thanks for including @stemsocial as a beneficiary, which gives you stronger support.
💕
Very interesting post. I enjoyed reading about the various biomarkers and the drugs. Although I wished there were more details associated with the drugs. But I understand that you can't cover it in one post.
On a separate note I have been thinking that almost everything you can think of from genetics to diet to psychological stress is a risk factor for CVD. What I was wondering is that if there is a common crossover point psychologically on how they all lead to CVD (for instance inflammation).
Affirmatively there is. Though I highlighted it in the previous article prior this but didn't expatiate it. However, now I have to.
Psychology actually has a huge link to cardiovascular disease. Most Psychological factors that have been known are mainly stress, anxiety, depression, and coping styles have been associated with an increased risk of cardiovascular disease.
They actually can contribute to the development of cardiovascular disease because they affect the individual's behavior and lifestyle, as well as biological processes such as inflammation and hormonal regulation. Someone who is emotionally depressed for example can decide to be withdrawn from the general society, engage sedentary lifestyle that can further complicate issues.
Naturally happiness is has a way of releasing wellness hormones like endorphins. The reverse is the case in depression state, anxiety and worries release stress hormones like the cortisol which is a catabolic hormone.
Psychology do have a role for sure.
Thanks for these lovely contribution.