Pathophysiology of Ulnar Neuropathy
Have you laid on your hands overnight, only to see that in the morning, you are unable to move your fifth finger (the pinky finger)? You might feel some tingling or numbness but over time, it would go away. That is just a simple case of your ulnar nerve having a slight pressure against it. This case can be severe in some people causing them to visit the hospital and possibly get surgery, and that case is known as Ulnar neuropathy. So in this post, I will be discussing Ulnar neuropathy.
Ulnar Neuropathy, also known as cubital tunnel syndrome is a mononeuropathy that involves the ulnar nerve. The Ulnar nerve is a nerve found at the upper extremities causing numbness in the pinky region of the hand which also spread to the ring finger. This condition isn't rare, it is a relatively common condition being one of the most common nerve entrapment conditions of the upper limb and forearm. This condition affects males more than females, with an increase in prevalence when a person gets to about age 35 years.

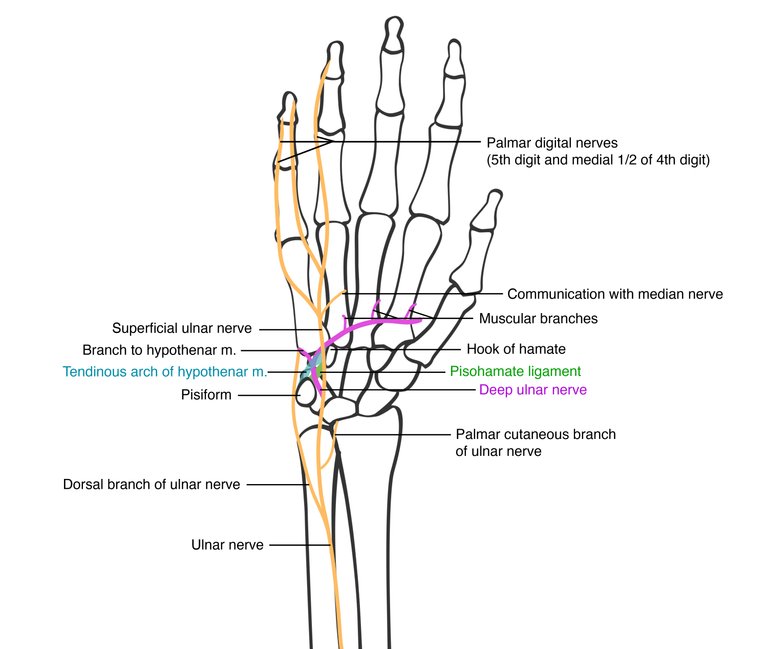
The Ulnar nerve comes from the neck through the arm and then to the medial aspect of the upper limb towards the wrist. It is a major peripheral nerve of the upper limb derived from the brachial plexus and a continuation of the medial cord. Ulnar is responsible for sensations of the anterior and posterior medial half of the fourth digit towards the fifth digit and it is responsible for sensations of the fifth digit and the ulnar aspect of the hand. Asides from sensation, it also performs motor functions as it innervates the muscles of the hand. It also innervates the flexor carpi ulnaris muscle in the forearm, and it also innervates the medial half of the flexor digitorum profundus. When this occurs, there will be numbness and loss of sensation in those areas, and this is a result of entrapment of the ulnar nerve which can occur at the elbow, the epicondylar/ulnar groove, and in the cubital tunnel. An entrapment can also occur at the canal of Guyon in the wrist and it can also occur at the forearm.
{kind=link}
{kind=link}
Ulnar neuropathy could occur as a result of direct pressure to the Ulnar nerve either in the process of sleeping in a wrong position that causes pressure to the placed on the nerve. Also, sitting positions, and resting on the elbow can be a very good reason to have ulnar neuropathy. Ulnar neuropathy can also be a result of a compression of the nerve during a medical procedure. It can also be from a condition such as Rheumatoid arthritis, Osteoarthritis, Blunt Trauma, Ganglionic cyst, and Tumors. Some other risk factors for Ulnar neuropathy are smoking, alcoholism, and bronchial artery occlusion.
Ulnar Neuropathy comes with Paresthesia which is the numbness and tingling of the medial half part of the 4th finger and the entire 5th finger. Patients will experience shooting pains, muscle pain, muscle Atrophy, and inability to grip properly. To evaluate the nerve injury, testing the flexion of the wrist requires having the patient flex the flexor carpi ulnaris against resistance in an ulnar direction. The Flexor digitorum profundus is tested as the fifth finger is pushed against resistance. Also, testing the Abductor digiti minimi is done by asking the patient to abduct the fifth finger against resistance. The first dorsal interosseous muscle is also tested by abducting the index finger against resistance. Blood work can be done to check for underlying causes such as hypothyroidism, anemia, and diabetes. Checking ANA for any case of autoimmune disease, Radiographic imaging of the elbow, the wrist, and the arm to check for bone spurs, valgus deformity, shallow olecranon grove, bone lesions, and tumors. An Ultrasound, MRI, and Electromyography can be done to look for changes in nerve diameter. If this is diagnosed, Non-Steroidal anti-inflammatory drugs are administered, Sleeping positions are changed, TCA antidepressants, Use of Elbow pads, Night Splinting, and the use of Splints. Surgical treatment can be done such as ulnar decompression in situ with anterior transposition, medial epicondylectomy, and endoscopic cubital tunnel release
Reference
https://www.ncbi.nlm.nih.gov/books/NBK534226/
https://www.uptodate.com/contents/ulnar-neuropathy-at-the-elbow-and-wrist
https://emedicine.medscape.com/article/1141515-overview
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4896870/
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0243324
Thanks for your contribution to the STEMsocial community. Feel free to join us on discord to get to know the rest of us!
Please consider delegating to the @stemsocial account (85% of the curation rewards are returned).
Thanks for including @stemsocial as a beneficiary, which gives you stronger support.