Acute Appendicitis in Pediatrics: Review of the topic + Clinical Case.
Acute appendicitis is the most frequent surgical pathology during childhood, so it represents the main diagnosis that should be ruled out in a child who consults for abdominal pain of sudden onset and of great intensity.
This clinical picture is based on the inflammation of the cecal appendix, generally caused by the obstruction of its lumen, which will lead to a process of various events, ranging from proximal and distal ischemia, and the intestinal wall necrosis; and if this process does not stop, it can reach the perforation of the organ and the wall adjacent to it.
It's for these reasons that acute appendicitis is a surgical emergency, which should be diagnosed and treated as soon as possible, in order to avoid its possible complications.

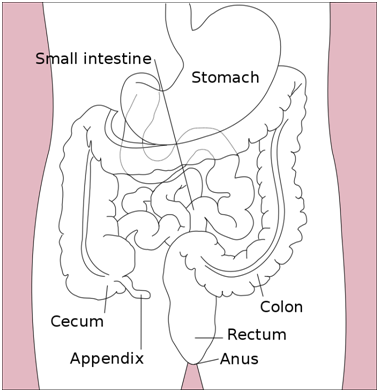
Before entering into the discussion of the pathological and surgical process of this organ, it's important to address certain basic aspects of the normal anatomy and physiology of the appendix, since they serve as the basis for many of the main characteristics of this inflammatory disease.
This organ is part of the digestive tract, serving as a place of reserve for certain wastes and bacteria of the intestinal flora and, although for a long time (and erroneously) it was believed that it was a vestigial organ that had no vital functions, it is currently known that it's actually an immune organ that actively participates in the secretion of immunoglobulins, in particular immunoglobulin A (IgA).
The appendix accompanies the cecum in all its incursions, and is implanted in the most cases, in the right iliac fossa, although in patients with intestinal malrotation, it can be located outside its usual location; In addition to this, we see how although the base of the appendix is implanted next to the cecum always, its body and its tip can have different anatomical locations, the most frequent being the retrocecal (behind the cecum), followed of the pelvic and laterocecal. An important anatomical reference when it comes to surgically locating the appendix is the three tapeworms of the colon, which converge at the junction of the appendix and the cecum. And the length of the organ can vary from less than 1 cm, to 40 cm (with an average of 6-9 cm).

As already mentioned, this pathology consists of the inflammation of the appendix, which can occur in people for various reasons. It has been proven that around 7% of the population will suffer from appendicitis throughout their lives, with the most frequent pediatric ages between 6 and 10; as for the gender ratio, it's slightly more frequent in men; and the mortality rate of this entity is very low (just 0.1%), however, it can reach 5% in newborn and nursling patients, where perforation complications are more frequent due to the delay in diagnosis in such young children.
In the same way, we see how there are certain risk factors that are considered as predisposing elements for the development of appendicitis during childhood, among them are:
The family predisposition, and it's important to clarify at this point that we are NOT talking about genetic predisposition, but family. How is this? Well, very easy, we see how in many cases of appendicitis the eating habits constitute a risk factor, because of their high carbohydrate and saturated fat content, as well as low fiber content, and this contribute to the formation of fecalites that obstruct the appendicular lumen; and the family customs causes this clinical situation to be repeated in members of the same family, since they usually share eating habits.
Age: the incidence in children under 3 years is very rare, having a maximum peak in the pediatric age between 6 and 10 years old; which decreases and increases again at age 15 until adulthood (it's believed that this is due to atrophy of the lymphoid tissue found in the appendix, which begins to atrophy and decrease from that age on).
Parasitosis by ascaris and other parasites (they lodge in the organ, obstructing their lumen).
Infectious processes: either viral or bacterial, they produce an increase in the lymphoid tissue of the appendix, which could cause the obstruction of its lumen; many times the acute appendicitis is preceded by a viral process about 2 weeks before its onset.
Hirschsprung disease: predisposes to the development of the disease in neonatal patients.
Tumors: the appendix constitutes the main organ in the digestive tract that serves as a seat for benign tumors, which can obstruct its lumen and develop the inflammatory process.
And as for the etiology of this pathology, in addition to the factors already explained above, this clinical picture has been related directly to certain concomitant situations or diseases, for example: intestinal obstructions, presence of fecalites and seeds in the digestive tract, intestinal parasites, tumors, fibrous bands, lymphoid tissue hyperplasia around the appendix, and incarceration of the hernia sac.
There are also special situations linked to specific pathologies:
Focal appendicitis --> Viral ulceration or bacterial overgrowth.
Contiguity appendicitis --> Piosalpinx.
Appendicular torsion --> Abdominal trauma.

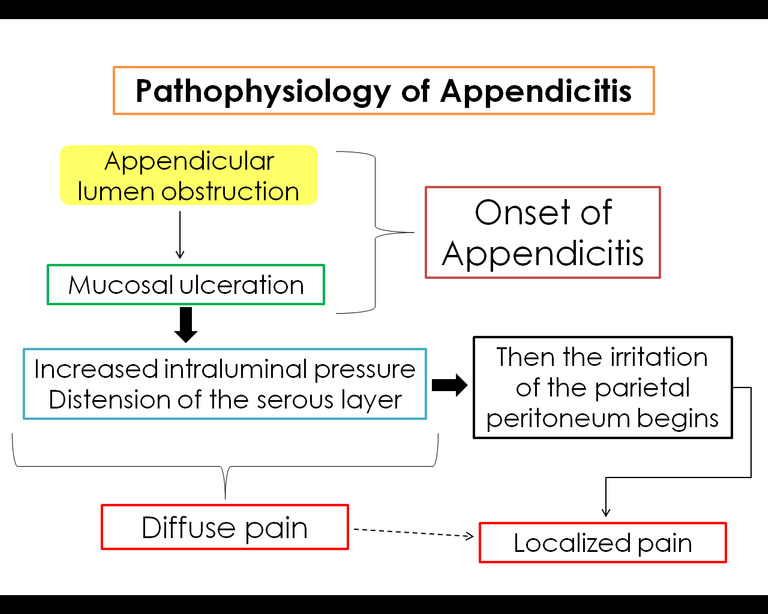
To understand a little better the process of development of this disease, and the consequent appearance of clinical signs and symptoms, it's important to explain the pathophysiology of the process:
It all starts with the obstruction of the lumen of the appendix, which can be caused by the presence of fecalites, parasites, foreign bodies, or excess lymphoid tissue, this obstruction causes intestinal stasis with bacterial accumulation and increased intraluminal pressure; consequently to this process the distension of the walls begins (which causes the diffuse pain that starts the clinical picture).
This inflammatory process causes the venous and arterial flow of the organ to decrease, leading to ischemia of the mucosa, which is invaded by microorganisms and their toxins (their absorption produces the appearance of the signs of tachycardia, fever and leukocytosis).
If the infection is not controlled, it soon invades the following layers of the appendix that are found immediately after the mucosa (serous and parietal peritoneum), and once the latter is affected, the irritation causes localized pain directly in the right lower quadrant.
In this way we see how all the pathogenic events related to the appendicitis picture go hand in hand with the appearance of the typical and known symptoms of acute appendicitis.
And finally, if the progression of the condition goes on, and the intraluminal pressure continues to increase until blood pressure is exceeded, this can cause infarctions of the mucosa and other layers, developing the perforation of the appendix, which is one of the complications that is most sought to avoid, since it involves an increase of bacterial proliferation in the abdominal cavity, and could lead to even more feared systemic complications.
In the following scheme the explanation was simplified for a better understanding:

To explain the presentation of this clinical picture, it's necessary to explain what has been known as the Murphy's Appendicular Chronology, in honor of the doctor who carried out the pertinent investigations to give the explanation for this flowery picture of manifestations.
This chronology is based on trying to explain the clinical manifestations that a patient with appendicitis presents, following the order of the pathophysiological events previously explained; In this way we see the pain, as the cardinal symptom of appendicitis, since it's present in all patients (although it can vary from both its character and its intensity).
Thus we see that in a FIRST PHASE, it's a generalized pain throughout the abdomen, or located at the level of epigastrium, and that is characterized by being visceral, diffuse and persistent (the characteristics of this pain are based on the fact that it occurs due to the distention of the walls due to visceral nerve stimulation); In addition to this, the patient usually presents anorexia or weight loss, nausea and vomiting (these begin as a reflex mechanism before inflammation of the appendix, and subsequently remain as a result of peritoneal inflammation); and the presence of fever that appears after 2 hours of the onset of the condition (occurs as a consequence of the invasion of the mucosa by bacteria, and the absorption of its toxins into the bloodstream), so in addition to increasing the temperature, leukocytosis it's develops at this level.
In a SECOND PHASE of the pain, it becomes located, at the level of the right iliac fossa (this pain is caused by peritoneal irritation, which becomes increasingly intense, and so this way the localized pain suppresses the delayed epigastric).
In summary, the main clinical features that we will find in a patient with acute appendicitis can be simplified in the Appendicular Triad of Dieulafoy:
- Cutaneous hyperesthesia.
- Abdominal pain
- Muscle contraction at the level of the right iliac fossa.

To carry out the diagnosis of this surgical emergency, it's important to take into account all aspects: clinical, imaging and laboratory tests.
- Physical Exploration:
We can observe certain typical characteristics in the patient, such as: "sick child" aspect, position or anti-pain gait, in which, to avoid pain the child usually flexes his body on the abdomen. And in addition to this, certain clinical signs such as fever, tachycardia, rapid and superficial pulse.
On the other hand, abdominal physical examination is essential to make a proper clinical diagnosis:
At Inspection, the presence of a large appendicular mass can be observed in some cases; and in cases where an appendicular abscess has developed, signs of phlogois (redness, increased volume) will also be observed.
At Auscultation, due to the presence of inflammatory paralytic ileus, hydro-noise is diminished.
At the Palpation it's important the presence of pain, its location, and evaluate a series of signs and maneuvers characteristic of specific surgical processes:
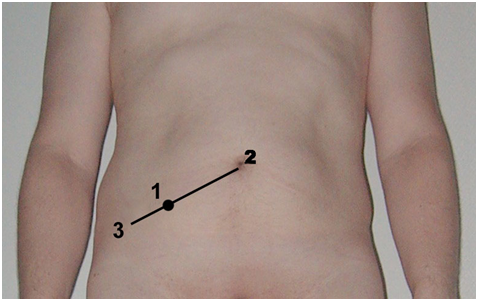
- Mc-Burney Point: it's an abdominal point that is obtained by drawing an imaginary line between the upper right iliac spine and the navel: if there is pain when palpating at this point, we're in the presence of a positive Sign of Blumberg, which is very common in cases of acute appendicitis.
Involuntary muscle defense: Indicates peritoneal irritation.
Cutaneous hyperesthesia: an exaggerated increase in sensitivity in the skin of the abdomen as a result of the inflammatory process.
- Voluntary muscular contracture: is characteristic of the simple phase of the picture.
Other Signs and Maneuvers to evaluate:
- Gueneau Mussey Sign: pain to decompression throughout the abdomen.
- Rovsing Sign: the pressure exerted on the lower left abdominal quadrant causes pain in the right quadrant (due to gas drainage).
- Dunphy Sign: coughing pain (due to increased intra-abdominal pressure).
- Psoas Maneuver: the patient lies in the supine position (face up) while the examiner slowly flexes his right thigh (its function is to make the psoas muscle rub the inflamed appendix, where the result would be a very painful response)
- Shutter Maneuver: In the same way the patient is lying supine, and when asked to flex and rotate the hip towards the midline of his body, a painful response is obtained if it's positive.
- Images:
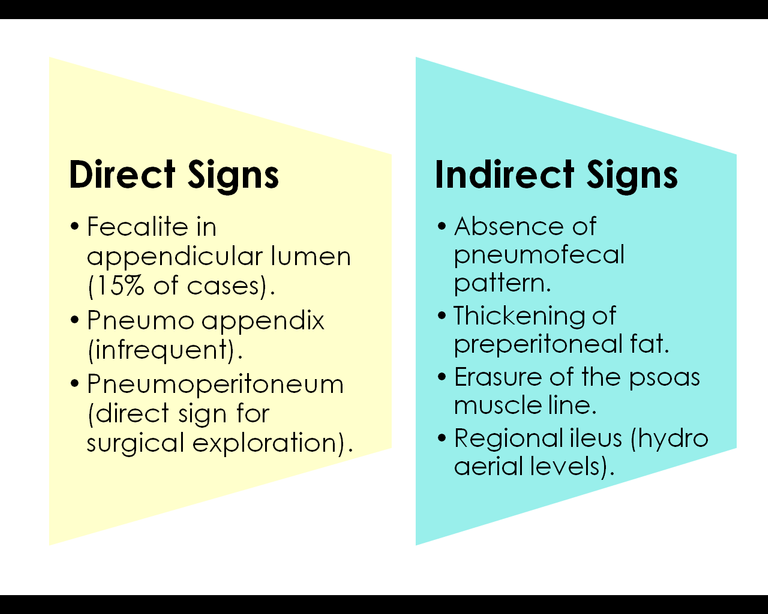
The imaging examination par excellence in the diagnosis of acute appendicitis is the Abdominal Radiography, where certain characteristic signs of this pathology can be observed. These signs have been classified as direct and indirect, depending on the specificity they have for this clinical picture, compared to other different abdominal processes.
Additionally, an abdominal ultrasound can be performed (it allows to rule out ovarian pathology; and in cases of appendicitis it can confirm the diagnosis when thickening of the organ wall is observed).
- Laboratory:
In a patient where the presence of appendicitis is suspected, the following laboratory tests will be requested:
Complete hematology (where moderate leukocytosis is observed in 80% of cases, and ** neutrophilia ** in 95% of them).
Uroanalysis (the existence of a urinary tract infection should always be ruled out).
The rest of the exams that are more specific to other pathologies, and that usually take an acute surgical abdomen, will be requested based on the diagnostic presumption.
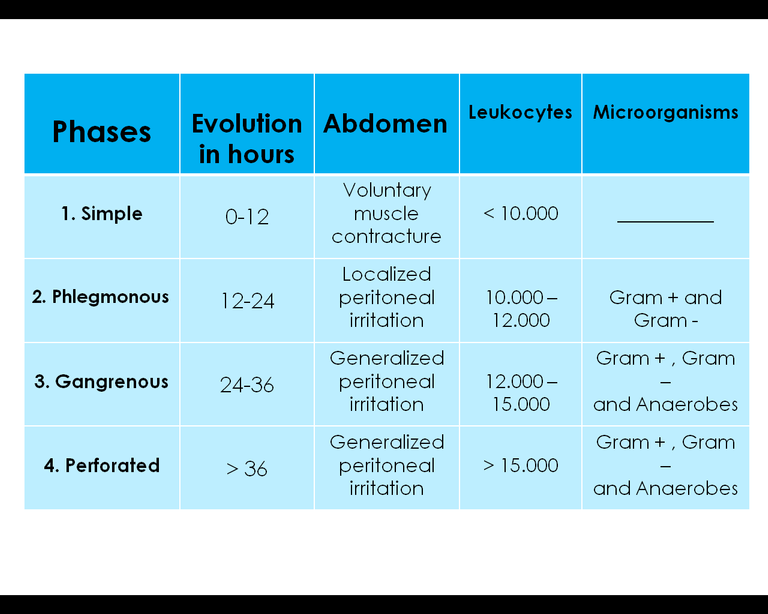
Another important characteristic of appendicitis is the fact that according to the clinical, pathological and laboratory characteristics of each patient, 4 phases can be clearly distinguished in the evolution of the disease; These are explained in the following table:
As for the definitive treatment of this pathological entity, it is the surgical: Appendicectomy; prior to which the hemodynamic stability of the patient must be ensured, correct the hydro-electrolyte imbalance, give symptomatic treatment for pain, and meet all those needs that each patient may present individually.
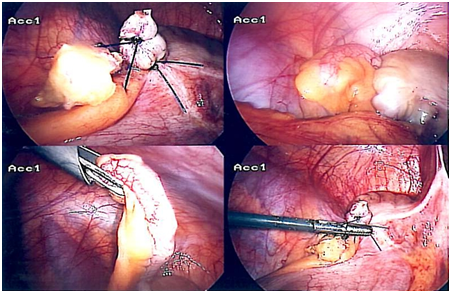
The surgery can be carried out either by conventional technique, that is to say open through an incision in the abdominal cavity, or by less invasive technique by laparoscopy.

{kind=link}
{kind=link}
{kind=link}

This is a 6-year-old female patient, without significant pathological or personal history, who consults for abdominal pain of sudden onset and strong intensity, which began in epigastrium and then focused on the level of the right iliac fossa, accompanied by vomiting in number of 3 and nutritional content, increase in body temperature quantified to 38.6 ° C and malaise.
The physical examination shows cutaneous hyperesthesia in all quadrants of the abdomen, as well as pain to decompression at Mc-Burney's point (positive Blumberg sign); laboratory paraclinics are requested that show results of leukocytosis at the expense of segmented cells; Therefore, behavior is decided: surgical intervention for appendectomy.
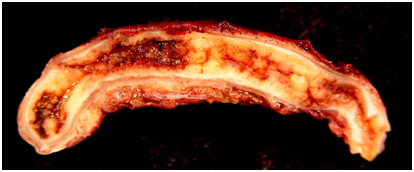
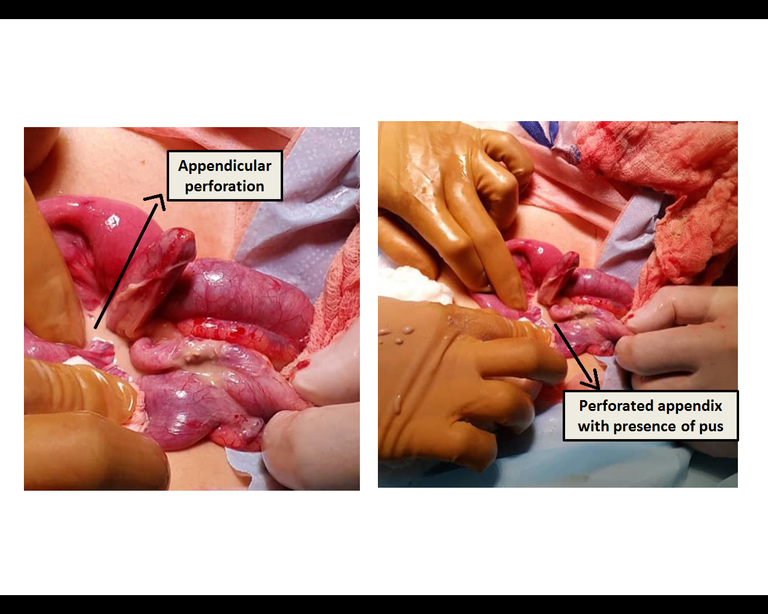
Among the surgical findings are: vermiform or perforated cecal appendix, with moderate amount of free pus in the abdominal cavity, which is extracted successfully, and the purulent secretion cavity is cleaned. Images of the moment of surgery are attached:
A satisfactory evolution was obtained with a patient discharge 48 hours after the surgery, with adequate medical indications for the specific case. These measures included broad-spectrum antibiotic treatment to prevent bacterial proliferation due to organ perforation and the presence of pus in the abdominal cavity; as well as rest, proper diet and symptomatic treatment for pain.
- Note: The images of the surgical procedure are the author's own, edited using the Microsoft Paint program.
CONCLUSIONS:
Acute appendicitis is one of the most frequent surgical emergencies at present day, with an increase in its appearance in pediatric age due to modifiable factors such as diet, or the presence of pathogenic microorganisms like intestinal parasites, therefore a good promotion of health is essential to start trying to reduce the prevalence of this pathology.
This clinical picture develops from a series of events that begin with the obstruction of the lumen of the appendix, which can be caused by various causes. The typical presentation consists of a picture of: severe abdominal pain, fever, nausea and vomiting, and increased white blood count. The diagnosis should be carried out as soon as possible, to achieve medical and surgical treatment (the latter being the definitive treatment), timely and effective.
Bibliographic references:
[1] Topics of Pediatric Surgery - Jesús Fernández.
[2] Pediatric Surgery - Ashcraft & Hollder.
[3] Principles of Surgery - Schwartz 10th Edition.
[4] Abdominal Operations - Rodney Maingot 11th Edition.
[5] Surgery: Fundamentals for clinical-surgical practice - Mariano E. Giménez.
Greetings again dear community of Steemit, especially to the scientific communities, for your constant support for the content I share with you all; On this occasion I wanted to present this article based on the frequency of this pathology in our environment, and it seemed to me that a good approach to the subject, and the presentation of a clinical case was the best way to explain the topic for a better understanding. It's always a pleasure for me to share medical content with all of you. Until next time! :)

Hello,
Your post has been manually curated by a @stem.curate curator.
We are dedicated to supporting great content, like yours on the STEMGeeks tribe.
Please join us on discord.
Thank you so much!
Congratulations! Your post has been selected as a daily Steemit truffle! It is listed on rank 2 of all contributions awarded today. You can find the TOP DAILY TRUFFLE PICKS HERE.
I upvoted your contribution because to my mind your post is at least 4 SBD worth and should receive 213 votes. It's now up to the lovely Steemit community to make this come true.
I am
TrufflePig, an Artificial Intelligence Bot that helps minnows and content curators using Machine Learning. If you are curious how I select content, you can find an explanation here!Have a nice day and sincerely yours,
TrufflePigThank you so much for the support :)
Hi, thanks for the post! I have included a link and a short description in my daily Science and technology digest, and you'll receive a 10% share of that post's rewards.
Hello, thank you for the support!
This post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @minnowbooster.
If you appreciate the work we are doing, then consider supporting our witness @stem.witness. Additional witness support to the curie witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Please consider using the steemstem.io app and/or including @steemstem in the list of beneficiaries of this post. This could yield a stronger support from SteemSTEM.
Thank you very much for the support! :)